The following explanatory notes are provided to give more detail on some of the issues raised in Parts I and II.
Note G(i): Respiratory illness
Studies have increasingly found significant relationships between respiratory illness risk and a bacterial indicator. This has been shown in recent studies in at least four different countries, but it may not be a new phenomenon:
- Hong Kong (Cheung et al 1990)
- England (Balarajan et al 1989; Fewtrell et al 1992; Fleisher, Kay, Salmon et al 1996)
- Australia (Corbett et al 1993)
- New Zealand (McBride, Salmond et al 1998).
The aetiological agent(s) for this are unclear, although it is generally recognised that a number of bacterial and viral pathogens that cause respiratory illness (e.g. members of the enterovirus and adenovirus group, and certain species of the genus Klebsiella) are shed in faecal matter. Infection is generally acquired by inhalation of aerosols containing these infectious particles (Horwitz 1990; Melnick 1990; Tyler & Fields 1990; Grimont et al 1992), and the potential for transmission of viral pathogens via wave-generated aerosols has been demonstrated (Baylor et al 1977).
Note G(ii): Examples of health risks
Contact with contaminated recreational water has been shown to pose a number of possible health risks. These illnesses, symptoms and pathogens are listed in Table G1, along with the relevant references.
A number of New Zealand cases of campylobacteriosis from the ingestion of contaminated drinking water have been demonstrated (Briesman 1987; Stehr-Green et al 1991; Ikram et al 1994; Eberhart-Phillips et al 1997), as has also been shown for giardiasis (Fraser & Cooke 1991). With respect to respiratory symptoms, inhalation of aerosols has been indicated as a possible transmission route (Baylor et al 1977; Tyler & Fields 1990). See also Note G(i).
Table G1: Bathing-related illnesses, symptoms and pathogens, with relevant references
| Illness/symptoms | Pathogen | Reference |
|---|---|---|
| Campylobacteriosis – acute diarrhoea with risk of dehydration lasting about five days, but may be longer. Usually with fever, headaches and nausea in the first stages. Abdominal pain can be sufficiently severe for patients to be hospitalised with suspected appendicitis. | Campylobacter jejuni | Koenraad et al. 1997 |
| Cryptosporidiosis – acute diarrhoea. Symptoms may wax and wane but duration in healthy persons is usually less than 20 days with spontaneous complete recovery. May be fatal in immunocompromised patients. | Cryptosporidium parvum | Sorvillo et al. 1992 |
| Ear infection – otitis externa, skin infection of the outer ear and otitis media, inner ear infection with exudate and earache. | Not identified (usually Pseudomonas aeruginosa, Streptococcus, and Staphylococcus) | Robson & Leung 1990 |
| Enterovirus-like illness – vomiting, diarrhoea, and abdominal pain. | Enteroviruses (type not identified) | D'Alessio et al. 1981 |
| Hepatitis A – long incubation with symptoms developing gradually. Symptoms include loss of appetite, malaise, fever and vomiting followed by jaundice. | Hepatitis A virus | Bryan et al. 1974 |
| Norwalk gastrointestinal illness – usually sudden onset with vomiting, diarrhoea and abdominal pain. Vomiting frequently appears without warning and may be projectile and uncontrollable, while diarrhoea may be explosive. | Small round structured viruses (SRSVs), including Norwalk virus | Barron et al. 1982 |
| Respiratory illness – cold and flu-like symptoms. May be associated with fever. | Adeno virus and others not identified | McBride, Salmond et al. 1998; Corbett et al. 1993; Fattal et al. 1986 |
| Shigellosis – diarrhoea that may vary from relatively mild to violent, with abdominal pains and fevers. | Shigella sonnei | Rosenberg et al. 1976 |
| Swimmer’s ear – otitis externa, infection of the outer ear. | Not identified (usually Pseudemonas aeruginosa) | Calderon & Mood 1982 |
| Typhoid and Paratyphoid (enteric) – fever | Salmonella typhi and Salmonella paratyphi | PHLS 1959 |
Note G(iii): State of the Environment Reporting
Environmental performance indicators are designed for use in state of the environment monitoring programmes. They help us to:
- systematically report on the state of New Zealand’s environmental assets
- systematically measure the performance of its environmental policies and legislation
- better prioritise policy and improve environmental decision making.
Over time, the information produced by State of the Environment reporting can:
- contribute to raising the level of knowledge about the state of New Zealand’s environment
- increase our ability to report on environmental health and trends
- provide the tools for effective evaluation of policy
- provide the information base for more informed policy and management decisions.
This document serves as a monitoring protocol two state of the environment performance indicators developed by the Ministry under the Environmental Performance Indicators (EPI) Programme. Please note that beaches refer to both freshwater and marine recreational areas, so each of the following indicators would be reported for marine and freshwater beaches:
- the percentage of monitored beaches in each beach grade
- the percentage of the season beaches or coastal areas were suitable for bathing or shellfish gathering.
Note G(iv): Pressure-State-Response model
The Pressure-State-Response (PSR) model was used to measure environmental performance of management responses to develop environmental performance indicators. The PSR model asks three important questions:
- What are the pressures on the environment?
- What is the state of the environment?
- What is being done to manage changes in pressures or state?
Pressure indicators answer the first question by measuring the stresses from human activities (and natural variations) that cause environmental change. State indicators answer the second question by measuring actual changes or trends in the physical or biological state of the environment. Response indicators answer the third question by monitoring the effectiveness of policies or actions taken by people to reduce, prevent or mitigate undesirable change in the state of the environment.
The indicators on which these guidelines are based; percentage of monitored beaches in each beach grade, and percentage of the season beaches or coastal areas were suitable for contact recreation or shellfish gathering, are state indicators that provide general information on the public health risk presented by recreational waters. Pressure indicators would measure the surrounding land use and discharges to water to assist identification of potential causes of changes in water quality. Response indicators would identify management or policy changes at the regional or national level (for example infrastructural improvements, land use management policies, national environmental standards) to manage issues for recreational waters.
Implementation of integrated pressure, state and response monitoring provides a measure of the entire system in question and supports detection of policy gaps or opportunities for management improvements.
Note G(v): Integrating public health and state of the environment data
The purpose of the Microbiological Water Quality Guidelines for Marine and Freshwater Recreational Areas is to help control the public health risk from microbiological contamination in recreational waters, and to provide a framework for monitoring and reporting on the general health of beaches. Integrating the needs of both state of the environment and public health monitoring may present some challenges, but it is achievable.
Microbiological information is generated more intensively to keep stock of short-term variation that can affect the public health risk of water quality. This monitoring takes place on a weekly basis, although at times follow-up monitoring is required to identify the permanence of an identified guideline exceedance.
The purpose of state of the environment monitoring is to collect sufficient data to produce information on the general health of the environment. This information can then be used to measure how well our management practices, policies and laws are working, and whether environmental outcomes are being achieved. The beach grades generated through the combination of the catchment assessment and microbiological assessment provide state of the environment information to the public on the general condition of the recreational area with respect to public health risk. The microbiological information collected to assess the public health risk at the beach on a weekly basis is aggregated over five years to generate the Microbiological Assessment Category used in the beach grading process.
Note G(vi): Merging with existing microbiological programmes
Councils may monitor microbiological water quality for objectives other than public health reporting (e.g. land-use pressure, trends). Merging monitoring programmes can result in significant cost savings, though there are some issues to be aware of.
The following considerations should be made when merging programmes other than for public health reporting:
- Can the sampling requirements of both programmes be satisfied?
- Will the sampling locations be appropriate for both programmes?
See Box 4 for an example of merging programmes.
Box 4: Issues with integrating programmes
Council A’s existing microbiological monitoring programme has been specifically designed to monitor the effects of agricultural land-use. The sampling conditions (wet, dry) and the locations of those sites are important to determine trends over time and space. The monitoring requirements to meet these objectives are:
- monitoring sites that are representative of the catchment
- avoiding monitoring during or after storm events, to avoid skewing trends
- monthly sampling.
However, the public health programme as outlined in the Microbiological Water Quality Guidelines for Marine and Freshwater Recreational Areas has been designed for the protection and reporting of public health risk. This requires:
- monitoring at beaches that are used for contact recreation
- sampling at locations and times that most closely represents public exposure (this may include sampling during rainfall events)
- weekly sampling.
When the council attempted to satisfy the monitoring requirements of both programmes, it quickly became clear that there would be difficulties merging the two without the objective of one or both of the programmes being compromised.
Merging or adapting an existing state of the environment monitoring programme to report on public health risk requires careful design to ensure the objectives of both programmes are successfully achieved. The following solutions are suggested where monitoring objectives conflict.
- Separate monitoring programmes: this is not the most efficient solution, but the clearest way to preserve the integrity of both monitoring programmes.
- Integrate the programmes: design a joint programme taking advantage of overlaps, recognising the specific sampling requirements of each programme. This approach is more complex and may involve tagging data considered unsuitable to the differing objectives.
- Economise sampling efforts: use the catchment assessment and frequency of use to prioritise beaches that require weekly sampling for public health risk evaluation. These beaches will form the focus for meeting the public health objectives of the guidelines. The land-use pressure objectives could then be met by a less stringent sampling regime while maintaining important trend information.
Note G(vii): Different roles and responsibilities adopted around New Zealand
As part of determining a sensible and pragmatic approach to recommending an assignment of roles and responsibilities, the Ministry for the Environment investigated a number of scenarios operating around the country.
Scenario One: Integrated approach
- The regional council undertakes all beach monitoring in an area.
- When the alert level is exceeded, the territorial local authority carries out additional monitoring. Additional sampling is funded by the Medical Officer of Health.
- A sanitary survey is carried out when in alert mode II.
- When the action level is exceeded the territorial local authority carries out additional monitoring. Additional sampling is funded by the Medical Officer of Health.
- Investigation of nuisance is carried out by the territorial local authority.
- When in action mode, public notification is undertaken by the Medical Officer of Health (includes signage).
Scenario Two: Medical Officer of Health lead
- The Medical Officer of Health brings the regional council and territorial local authorities in the region together before the beginning of the bathing season to ascertain the degree of monitoring programmed for the region. The Medical Officer of Health is kept informed of the status of beaches throughout the entire season.
- The territorial local authority carries out all monitoring in each district.
- When the alert level is exceeded the territorial local authority undertakes a degree of investigation (additional sampling is rarely carried out).
- When the action level is exceeded signs are put up at beaches (sometimes permanent around some discharge points) and a public communications strategy is implemented.
- An investigation into the cause of nuisance is carried out.
- The regional council is kept informed throughout the season.
Scenario Three: Single agency
- The territorial local authority carries out monitoring.
- The public are not alerted when action levels are exceeded, although an investigation is carried out to find the cause of the problem and abate nuisance.
- The Medical Officer of Health is available to provide advice to the territorial local authority on whether to inform the public.
Scenario Four: Regional lead
- The regional council carries out all monitoring.
- Territorial local authorities remain informed of water quality in their district through regional councils.
- The Medical Officer of Health is informed by regional councils when the action level is exceeded, and provides advice on the public health significance.
- Regional councils take additional samples and investigate when the action level is exceeded.
- The Medical Officer of Health informs the public when the action level is exceeded.
Scenario Five: Double check
- The regional council monitors beaches for state of the environment reporting.
- The territorial local authorities monitor beaches for public health purposes.
- The Medical Officer of Health provides advice on a sampling strategy and the public health significance of sampling results.
- The territorial local authorities carry out additional sampling and investigation when alert levels are exceeded.
- Territorial local authorities inform the public when action levels are exceeded and investigate the nuisance.
Note G(viii): The legislative basis for the Ministry’s recommendations
The recommendations made by the Ministry for the Environment and the Ministry of Health are supported by legislation as follows.
The regional council undertakes surveillance and alert-level monitoring (including resource consent monitoring).
Section 35 of the Resource Management Act, 1991 requires regional councils to undertake monitoring to carry out their functions under the RMA effectively. Section 35(2) requires regional councils to undertake “state of the environment” monitoring.
Under the RMA, regional councils have functions in relation to the coastal marine area, including coastal waters, which are linked to the purpose of the RMA. The aspects of the purpose of the RMA (Part II) that are relevant to coastal waters/marine bathing and, in particular, the public health aspects of beach water quality are:
- section 5 – sustainable management incorporates health and safety, safeguarding the life-supporting capacity of water and avoiding, remedying or mitigating any adverse effects of activities on the environment
- section 6 – the preservation of the natural character of the coastal environment, including the coastal marine area and the maintenance and enhancement of public access to and along the coastal marine area are matters of national importance
- section 7 – the maintenance and enhancement of amenity values and the quality of the environment are matters to which particular regard must be had by decision makers under the RMA.
Section 30 of the RMA ascribes functions to regional councils for the purpose of giving effect to the RMA, including:
- control of land use for the purpose of maintaining and enhancing the quality of coastal water
- in respect of the coastal marine area, the control of discharges of contaminants into water and discharges of water into water
- the general, control of discharges of contaminants into water and discharges of water into water.
Policy 5.1.1 of the New Zealand Coastal Policy Statement directs regional councils that:
Rules should be made as soon as possible with the object of enhancing water quality in the coastal environment where that is desirable to assist in achieving the purpose of the Act, and in particular where there is a high public interest in, or use of the water.
In summary, it is consistent with the RMA to require regional councils to undertake surveillance monitoring and alert-level monitoring of marine bathing waters. Arguably, the RMA requires regional councils to go further than this and undertake stepped-up nuisance monitoring, where necessary.
There is no provision in the Health Act for the Medical Officer of Health to audit the monitoring carried out by regional councils. However, the recommendation that the Medical Officer of Health be satisfied with the manner in which the monitoring is carried out is to protect public health and safety. It also helps to ensure that the guidelines will be consistently applied around the country.
If alert or action levels are reached the regional council informs the Medical Officer of Health and the territorial authority. The Medical Officer of Health ensures the territorial authority is informed.
Section 35(2) of the RMA requires regional councils to “take appropriate action (having regard to the methods available to it under the RMA) where this is shown to be necessary”. This is linked to state of the environment monitoring requirements. Appropriate action may include informing the Medical Officer of Health and territorial authority.
Once the Medical Officer of Health is aware that alert or action levels have been exceeded, it is consistent with the Health Act that he or she ensure that the territorial authority is informed. Under the Health Act, the Director-General of Health (and his or her officers) has an overriding duty to improve, promote and protect public health. The Medical Officers of Health and Health Protection Officers under the Director-General of Health have supervisory/ auditing roles in relation to public nuisances. While there is specific legislative authority for the Medical Officer of Health to direct territorial authorities, there is currently no such authority for him or her to direct regional councils.
The territorial authority informs the public, where necessary. The Medical Officer of Health ensures the public are informed.
Territorial authorities have a duty to improve, promote and protect public health within their districts under section 23 of the Health Act. This extends to specific powers and duties:
If satisfied that any nuisance, or any condition likely to be injurious to health or offensive, exists in the district, the territorial authority is to cause all proper steps to be taken to secure the abatement of the nuisance or the removal of the condition.
“All proper steps” arguably includes informing the public. Also, as outlined above, the Medical Officer of Health has an auditing role under the Health Act, and it is consistent with this that he or she ensures that the public is informed.
Section 57 of the RMA provides for a New Zealand Coastal Policy Statement (NZCPS), which is mandatory. By virtue of sections 55 and 57, local authorities must take such action as is necessary to implement the NZCPS. Policy 5.1.7 of the NZCPS states:
Provision should be made to ensure that the public is adequately warned when the degradation of water in the coastal environment has rendered the water unsafe for swimming, shellfish gathering or other activities.
Consequently, the NZCPS directs local authorities to make provision to warn the public.
Regional councils have functions to ensure that integrated management of the natural and physical resources of a region is achieved, and provision could be achieved by ensuring that territorial authorities will carry out this function.
If the action level is reached, in the first instance the territorial authority will undertake nuisance monitoring and cause all proper steps to be taken to abate or remove the nuisance. On occasion it may be more appropriate for the regional council to undertake this duty. The Medical Officer of Health will provide advice and ensure that the territorial local authorities and/or regional councils take proper steps.
The Health Act requires territorial authorities to undertake nuisance monitoring in relation to their districts pursuant to section 23:
To cause inspection of its district to be regularly made for the purpose of ascertaining if any nuisances, or any conditions likely to be injurious to health or offensive, exist in the district.
‘District’ is not defined in the Health Act, and arguably the coastal marine area is not within a territorial authority’s district because of the definition of ‘district’ in the RMA. However, this definition does not expressly apply to the Health Act. Further, the source of the nuisance is likely to be within the territorial authority’s district (i.e. the land, as defined in the RMA), and it is appropriate that the territorial authority locate the source of the nuisance.
The RMA requirements for regional councils to monitor may extend to nuisance monitoring. For example, where the cause of the nuisance is found to be a consented activity or an activity controlled by the regional council rather than the territorial local authority, then responsibility for continued monitoring and abatement rests with the regional council. Other situations where it may be more appropriate for the regional council to carry out nuisance monitoring include when it has been agreed by all agencies involved before the beginning of the bathing season, and where the territorial local authority is too small to cope with increased monitoring. The Medical Officer of Health may need to assist the territorial local authorities and regional councils in determining the most appropriate agency to investigate and monitor the nuisance.
Note G(ix): Legal opinion on roles and responsibilities
A legal opinion sought by the Ministry for the Environment found that the two major pieces of legislation concerned (the RMA and Health Act) did not explicitly define responsibilities for beach water-quality monitoring and reporting. However, the proposed framework is consistent with current legislation.
Note G(x): The Annapolis Protocol
The Annapolis Protocol combines a monitoring scheme of microbiological testing with broader data collection on sources and transmission of pollution. It involves both an environmental hazard assessment and a microbiological water-quality assessment.
Councils and health authorities have been consulted on the concept and implementation of a risk-based approach and guideline values for recreational waters. The Annapolis Protocol framework as detailed in the guidelines has been adapted to suit New Zealand conditions after trial at 30 New Zealand recreational beaches and consideration by a Marine Bathing Working Group established for the purpose. The same approach has been applied to the guidelines for freshwater recreational use, following consideration and trial by the Freshwater Guidelines Advisory Group.
Note H(i): Sampling times and periods
Season period
The bathing season period will vary according to location, but will generally extend from 1 November to 31 March. If a beach is used all year round the grade and weekly monitoring should reflect this (i.e. should be based on data for a period relevant to usage).
A Suitability for Recreation Grade (SFRG) is established for each beach in the programme at the beginning of the season. The SFRG is applicable for up to five years, provided there are no significant changes within the catchment that might affect water quality. The grade provides an indication of the overall condition of the site.
Weekly sampling should continue at those beaches graded Good, Fair or Poor. Weekly sampling is required for determining the public health risk at a beach. Beaches graded Very Good may not require ongoing monitoring because of the low risk identified. The same applies to beaches graded Very Poor, as they will generally be unsuitable for recreational use.
Resource limitations may restrict the number of beaches in a region that can be monitored. The grading system applied in these guidelines enables beaches to be prioritised according to their grade, and creates the potential to have all beaches within a region, city or district graded over time.
Number of samples to collect
A minimum of 20 samples should be collected from each site in the monitoring programme, usually at weekly intervals. Additional samples may be taken throughout the season as a result of single-sample exceedances. While these do not contribute to the recommended 20 samples, they should be recorded in the database/spreadsheet with all other samples.
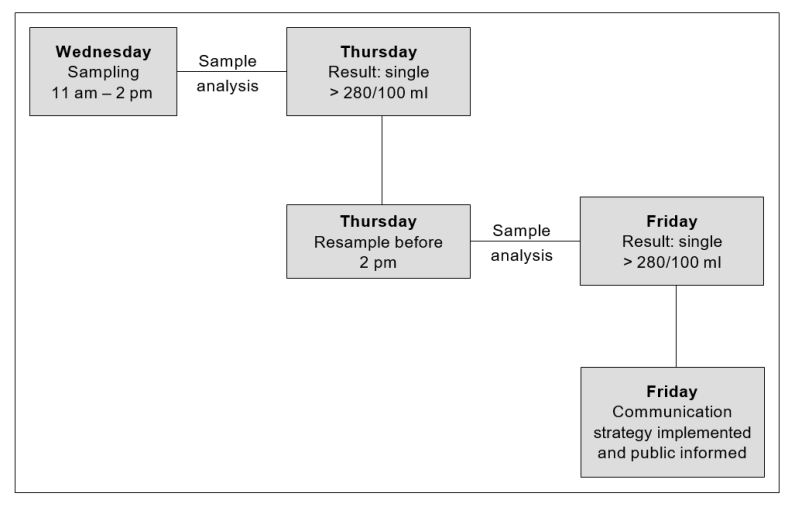
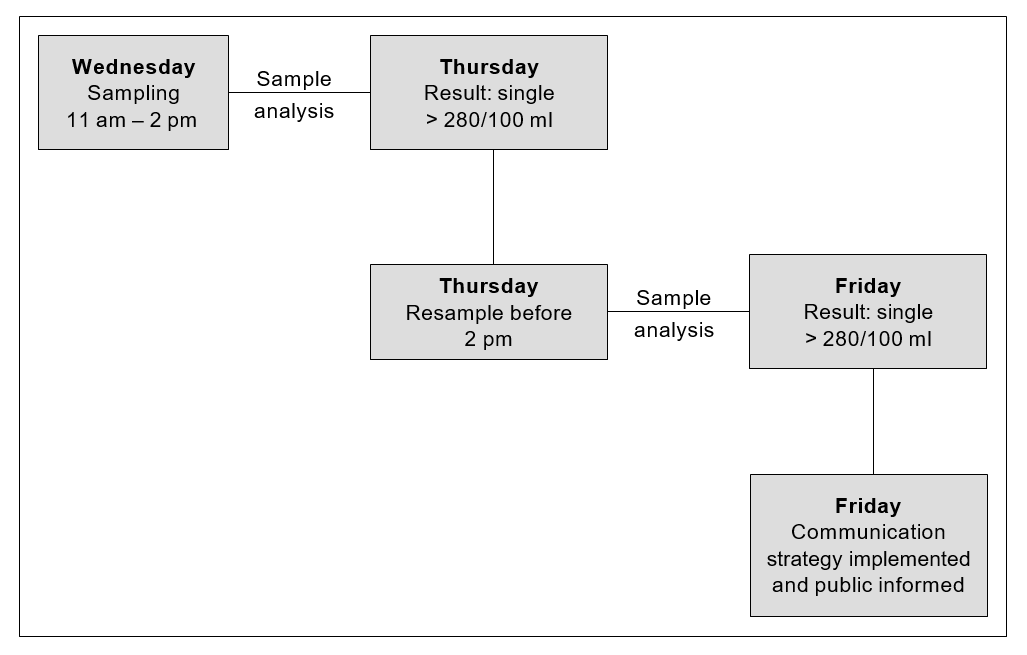
Timing sample collection
Figure H1 shows how a sampling regime may be timed. In this instance it ensures that the results are generated in time to inform the public of the quality of the beach at the time of highest use (the weekend). There may be other peak times when the regime in Figure H1 is not appropriate and staff should design programmes accordingly.
Flexibility in sample timing
In setting up a programme it is important to allow for the minimum number of samples to be collected (20). This will usually require weekly monitoring, depending on season period (which may vary from region to region). As sampling is not likely to take place during conditions which may present a health and safety hazard (e.g. heavy rainfall, storm conditions, large surf), it is important to design a weekly sampling programme that has sufficient flexibility to allow sampling to take place as soon as practical after adverse conditions have abated. This may also better reflect the conditions under which people are swimming.
Figure H1: Example of a proposed sampling strategy (marine waters)
24-hour re-sampling requirement
Marine waters
For marine waters when sampling returns a result exceeding the action level threshold, the guidelines require a follow-up sample within 24 hours of receiving the first result. The purpose of the follow-up sample is to ensure that the first sample is not an anomaly and that the problem is persistent before initiating a public notification plan.
Ideally, resampling should take place within 24 hours of receiving a high result. While this does not present a problem for urban beaches, logistically it may not be possible for more remote locations. In such instances re-sampling should take place between 24 and 72 hours after receiving a high result.
If a sampling agency has remote sites it may be possible to arrange for another organisation to collect samples and transport them to a local laboratory for analysis. Health agencies, territorial local authorities or community organisations may be able assist with sampling, and could be particularly useful for re-sampling in remote locations.
Freshwaters
No follow-up sample is required to confirm an exceedance of the alert-level threshold. There are two reasons for this: the dilution factor is likely to be less than for marine waters resulting in more extreme exceedances; and potentially higher concentrations and a greater range of pathogens may be present in freshwaters.
Note H(ii): Techniques for taking and analysing samples
Where to sample
Water-quality samples should be taken from the area where swimming occurs. In general, the sample will be taken at approximately 15 cm below the surface at a point where the depth of water is 0.5 metres for marine water, and 30 cm below the surface at a point where the depth of water is 1 metre for freshwater.
Multiple sample sites
Sometimes it may be desirable to take multiple samples along a beach, particularly where a beach extends for some distance and one sample point is not representative of the whole beach. The way multiple samples are incorporated into results will vary. If samples are taken at considerable distances from each other, then each of the samples should be considered an individual sample site. However, if multiple samples are taken from a small beach (e.g. with the purpose of trying to find a potential source of contamination), then these will need to be treated differently, and the highest value should be taken as the maximum for the whole beach.
Sample collection techniques
At the time of sampling, enter in a logbook (for later transcription to a sample sheet) details of weather conditions (wind speed and direction, rainfall), water temperature, salinity, and observations of conditions such as turbidity or discoloration, and any unusual circumstances affecting the site (e.g. seaweed, jellyfish).
The following steps for sampling are recommended.
- Ensure that the bottle is clearly labelled for later sample identification.
- Immediately before sample collection, remove the bottle cap while ensuring that the inner of the cap is protected from soiling. The laboratory generally supplies sterile containers of a suitable size.
- Quickly plunge the bottle upside down to the required sampling depth set for the site. (For marine water the sample will be taken at approximately 15–20 cm below the surface at a point where the depth of water is 0.5 metres; for freshwater the sample will be taken at approximately 30 cm below the surface where the depth of the water is approximately 1 metre.)
- Tilt the bottle until the neck points slightly upwards, with the mouth directed towards the current. The bottle can be moved forward horizontally until filled if necessary. Completely fill the bottle.
- Rapidly bring the bottle to the surface and pour out a small portion (leave a space of 2–3 cm) to permit proper mixing for analysis. Quickly fit the cap and secure tightly.
- Record the time of sample collection and check sample identification labelling.
- Place in a chilly bin containing frozen slicker pads.
Sampling after wet weather
The guidelines relate to samples taken throughout the total bathing season irrespective of weather conditions. Results influenced by rainfall should not be excluded: people do swim shortly after a rainfall event, and it is important to sample when people are likely to be swimming. This may be particularly so for freshwater lakes and rivers.
The separation of dry-weather and wet-weather data is also impractical because the definition of the two is problematic. For example, coastal water can be less polluted in the early stages of a wet spell but more polluted when the weather has become fine just after substantial rainfall; the reverse can be true in estuaries.
Safety
The safety of field officers is vital and should be taken into account when selecting sample sites with respect to entering the water.
Transporting samples
The sample should be transported to the analytical laboratory as quickly as facilities allow, preferably within six hours, but no longer than 24 hours.
When it is not possible to have the samples analysed by the local laboratory, a courier should be arranged well in advance. Courier companies can be requested to make a pick-up from the council in time to courier the samples to the laboratory on the same day or overnight. Samples should be packed in chilly bins (polystyrene bins are sufficient) with ice packs to keep them cool.
It is particularly important that samples analysed for E. coli are analysed within 24 hours of sampling, as bacteria may begin to die or replicate, depending on storage conditions and the status of the water sample.
Documentation of the transport history and of all those who have handled the sample should accompany all samples. This is known as a chain of custody.
On arrival at the laboratory the samples should be placed in a refrigerator, and analysed within two hours of receipt (particularly for enterococci and E. coli; different time factors may be applicable for other micro-organisms). The analytical laboratory should record the times of sample receipt and analysis.
Where analysis for other micro-organisms is required, obtain specific instructions from the analytical laboratory.
Laboratory techniques
Marine studies have generally concluded that enterococci are the indicator of choice for the presence of faecal pollution. The recommended method for their detection in the Recreational Water Quality Guidelines are the Membrane Filter (MF) Test Method for Enterococci in Water as described in Document No. EPA-821-C-97-004, and Enterolert™ (note: Enterolert™ may not be considered suitable for state of the environment monitoring and reporting due to inadequate detection limits).
The above method has been evaluated for marine waters and has the advantage of giving results in 24 hours. Earlier methods gave a result within 48 hours. The value of this for monitoring agencies is to be able to identify alert, and action-level exceedances more quickly.
For similar reasons, in freshwater where E. coli is the indicator of choice, Colilert™ and EPA method 1103.1, 1985 Membrane Filter Method for E. coli are the preferred methods to enumerate Escherichia coli. Both methods give a result within 24 hours.
Quality control
Laboratories conducting testing for monitoring agencies must be able to demonstrate competence. Ideally this means an IANZ accredited laboratory.
It is essential that laboratories have documented quality assurance procedures. This does not have to be in the form of very detailed manuals, but the basic procedures of the laboratory must be written down. It needs to be quite clear what procedures are being used and exactly how the tests are being carried out. All key activities must be documented, and everyone involved in testing – from sample collector to the person reporting the results – must have a thorough understanding of their responsibilities and duties, any problems that could arise, and how they should be dealt with. All activities undertaken must be recorded so that it is quite clear, from the time of collection of the sample to the reporting of results, what actions were taken, by whom and when.
In showing competence, laboratories need to consider participation in an inter-laboratory proficiency programme, spiked samples, split samples, duplicates, positive and negative controls, both within the laboratory and in collaborative tests with other laboratories.
New method validation
New methods must be proven to provide results equivalent in sensitivity and specificity to those of the preferred test methods for the waters being tested. Statistical analysis of parallel test results must show strong linear correlation and no significant difference between the methods by paired t-test analysis.
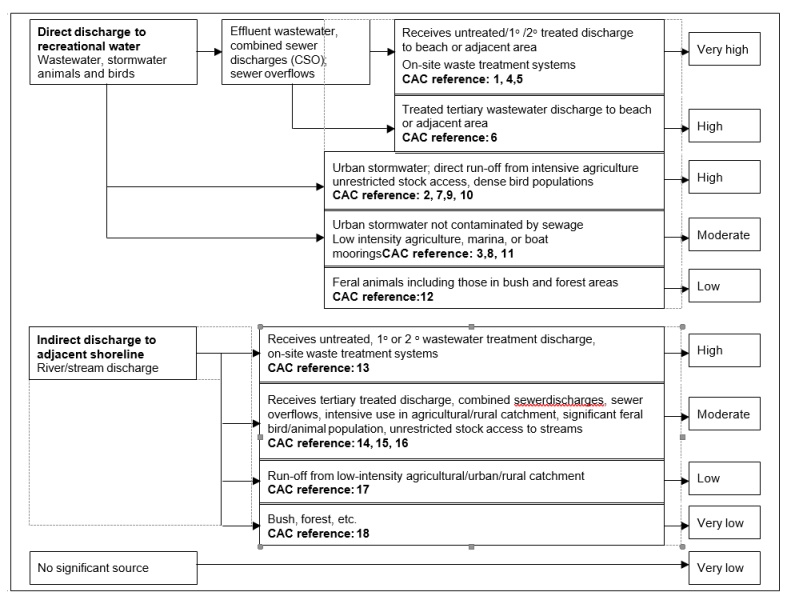
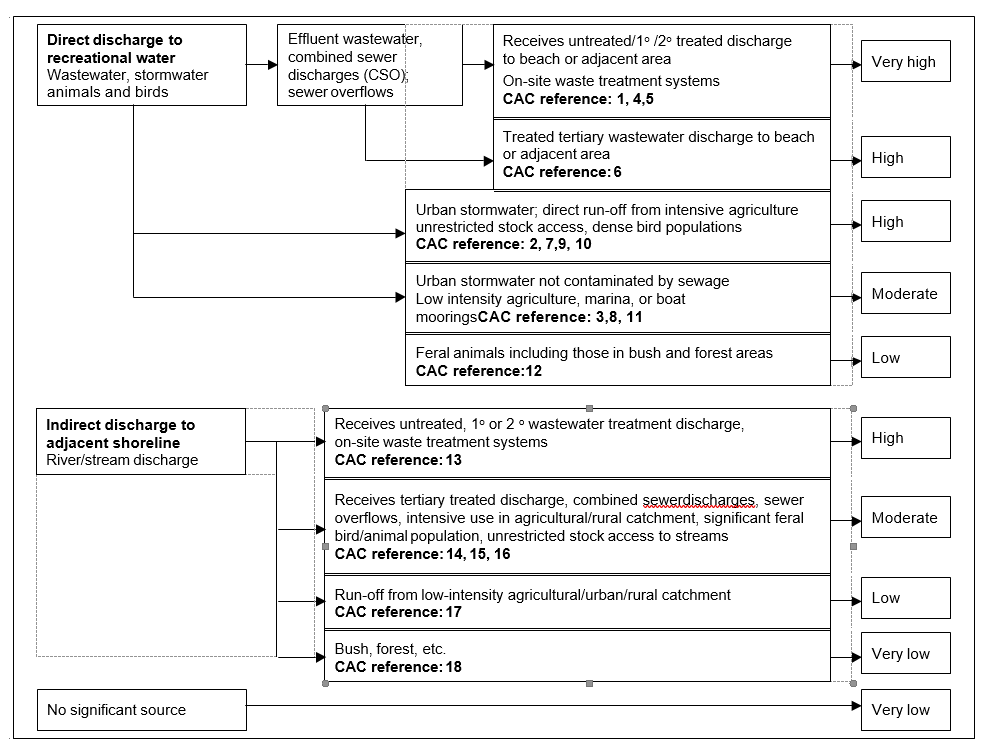
Note H(iii): Establishing a Sanitary Inspection Category (SIC)
The following steps are required to determine an SIC.
- Carry out an initial desktop analysis based on historical information.
- Use Parts A, B and C of the Catchment Assessment Checklist to help identify relevant information about the site.
- Use Part D of the Catchment Assessment Checklist to identify the presence of sources of faecal contamination likely to cause effects in the water body.
- If more than one source is present, then choose the most important. Importance is assessed in terms of the susceptibility of the water body to faecal influence. For example, a continual moderate source of faecal contamination may be considered more important than an occasional but high-load faecal source. This may require specific pathogen testing to determine the source of greater impact.
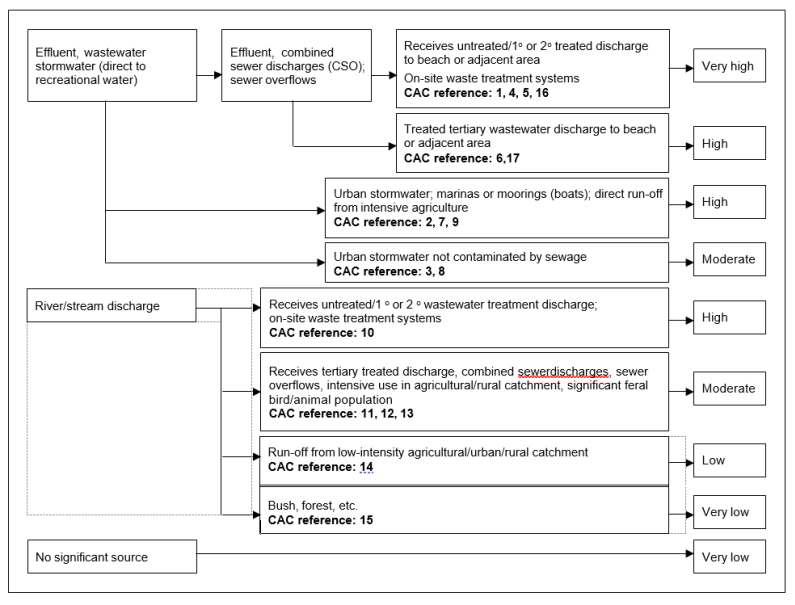
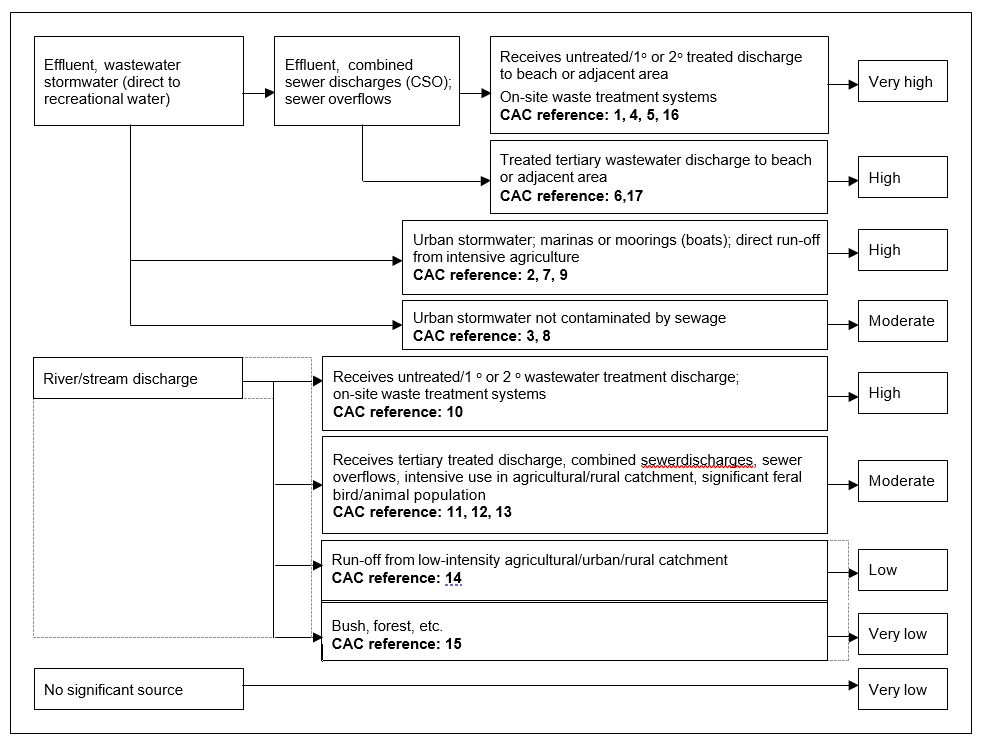
- Locate the number corresponding to the most significant impact in the SIC flow chart (Figure H2) to determine the SIC.
It is important to recognise there are two questions to be answered in Part D of the catchment assessment checklist. The first is “Is it present”. The purpose of this question is to determine the presence of a potential source of faecal contamination to the recreational site. The second question “Is it likely to cause an effect” determines, after evaluation, if the potential source of faecal contamination actually affects the recreational site, thus posing a risk.
Initial desktop assessment before sanitary inspection
Start the assessment of the sanitary status of a recreational site with a review of its previous history and, where applicable, an assessment of what triggers pollution events, including when and how the guidelines are exceeded.
When considering historical microbiological data to help determine causal relationships, bear in mind the limitations – under some conditions – of the indicator (enterococci/faecal coliform) used. Additional information, such as that set out in Parts A, B and C of the Catchment Assessment Checklist, may be needed to verify the cause of elevated indicator levels, and may already be available in the historical information.
Carrying out a sanitary inspection
Generally, local authorities will have GIS systems or maps to identify the important known discharges and conditions that could cause an issue. The initial emphasis of any assessment should be on potential causes from known discharges and existing conditions, identified using resource information, local data and historical information. In addition, identifying what is not known is important. Gaps in the knowledge about an area can be addressed in a catchment inspection, as well as by reviewing known existing conditions.
To assess the immediate area and catchment data, an annotated map of the beach and catchment is required. The checklist can be used to verify that all aspects and areas that should be included in the map have been added.
Questions that require information for annotation may include:
- number of bathers
- location of oxidation ponds
- duck ponds
- bird-roosting areas (daytime and night time)
- boat anchor and mooring areas
- possibility of septic tank seepage
- location of swamps and mangroves
- location of wastewater treatment and disposal systems and effluent outfalls.
Possible contamination sources (rivers, streams, stormwater drains outfalls) should be included in the map of the sanitary inspection area. Where available, maps of the entire catchment area indicating land use, topography and infrastructure networks (i.e. wastewater and storm drain systems etc.) should also be attached.
Base conditions for establishing a Sanitary Inspection Category
All beaches will have been recognised as having contact recreational activity, so a factor for human-to-human transmission of disease during recreational activity is not included. A single most significant source of faecal contamination has been used to categorise the beach. This is because a second source, even of similar magnitude, can only increase the risk by a factor of two and as such is of limited significance in microbiological terms.
Other impacts not included above may produce an ‘unexpected result requiring verification’ in the grading matrix (Tables D2 and E2). This source should be identified in the ‘more detailed investigation’ suggested in the note to Part D of the Catchment Assessment Checklist.
Note: The Sanitary Inspection Category (SIC) is based on the use of, and monitoring for, faecal indicator bacteria to support risk assessment. As discussed in the introduction, where there are discharges of treated effluent enterococci alone are not an appropriate indicator of public health risk. If pathogen monitoring is carried out then the SIC category for tertiary treated wastewater discharge may be amended.
Note H(iv): Catchment Assessment Checklist (CAC) for marine recreational waters
Catchment Assessment Checklist (CAC) for marine recreational waters [PDF, 277 KB]
Figure H2: Sanitary Inspection Category flow chart for marine recreational waters
Note H(v): Microbiological Assessment Category (MAC) for marine recreational waters
The Microbiological Assessment Category is calculated on the basis of five years of historical data (at least 100 data points). Data collected during or immediately following rainfall, as part of routine sampling, should be included in the calculation of the MAC. The purpose of the MAC is to give an indication of general water quality over an extended period, to allow for variations in climatic conditions. The MAC is used in conjunction with the Sanitary Inspection Category (SIC) to determine the Suitability for Recreation Grade, and to confirm that the selected SIC is accurate, based on historical water-quality results.
Note: Follow-up samples from an alert or action mode response should not be included in the data used to generate an MAC. If using the software provided by the Ministry for the Environment to generate grades, follow-up samples will need to be removed from the dataset prior to importing.
See Section D.3 for MAC definitions.
Change in indicators
If a change between indicators is made, there may be limited amounts of data available in the initial years of implementation. To overcome this, correction factors appropriate to local conditions can be applied to historical records. Such conversion factors would normally be based on the results of local analyses.
For many locations there will be a large amount of historical data available that can be used for preliminary recreational water environment classification. If this data includes analysis for enterococci, there will be no problem using the data. However, many recreational water environment managers will have data based only on coliform and faecal coliform counts. Although there is no exact relationship between enterococci and E. coli counts, a relationship expressed by the following equation (WHO 2001) may help in interpreting historical data:
- log10(faecal coliform) = 1.028 + 0.601log10(enterococci)
Even more helpful are the following simpler forms of this equation, relating enterococci to faecal coliforms and vice versa:
- faecal coliform = 10.67(enterococci)0.601
- enterococci = 0.0195(faecal coliform)1.67
Using the first formula, a count of 70 enterococci equates to 137.1 faecal coliforms. Using the second formula, a count of 100 faecal coliforms/100 mL equates to 42.7 enterococci/ 100 mL.
However, this equivalence is not exact as it is based on the relationship between faecal coliform and faecal streptococcal/enterococci counts in United Kingdom bathing waters after censoring zero values. If possible, local recreational-water environment managers should define the relationship that exists in their own waters.
Note H(vi): Suitability for recreation grade for marine recreational waters
Explanation of grades
Beaches are graded by considering microbiological monitoring results from previous years in combination with the factors in the catchment that may contribute faecal contamination to the beach. It is a risk-associated grading of the beach, meaning that it provides an indication of what the likely condition of the beach will be on any day. The following general explanation provides a description of each of the beach grades.
Very good
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have very good water quality (see Table D2 for details). There may be some run-off from low-intensity agricultural/urban/rural catchments, but there are likely to be no significant sources of faecal contamination.
Recommendation: Considered satisfactory for swimming at all times, and therefore may not require monitoring on a regular basis.
Good
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have generally good water quality (see Table D2 for details). On occasions (such as after high rainfall) there may be an increased risk of contamination from run-off. Such sites receive run-off from one or more of the following sources and may contain animal or human faecal material:
- river discharges impacted by tertiary treated wastewater, combined sewer overflows, intensive agricultural/rural catchments, feral bird/animal populations
- river discharges impacted by; run-off from low-intensity agricultural/urban/rural catchment
- stormwater not contaminated by sewage.
Recommendation: Satisfactory for swimming most of the time. Exceptions may include following rainfall. Such beaches are monitored regularly throughout the summer season and warning signs will be erected if water quality deteriorates.
Fair
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have generally fair water quality (see Table D2 for details). Events such as high rainfall increase the risk of contamination levels from run-off. Such sites receive run-off from one or more of the following sources and may contain animal or human faecal material:
- river discharges impacted by tertiary treated wastewater, combined sewer overflows, intensive agricultural/rural catchments, feral bird/animal populations
- river discharges impacted by run-off from low-intensity agricultural/urban/rural catchment
- stormwater not contaminated by sewage.
Recommendation: Generally satisfactory for swimming, though there are many potential sources of faecal material. Caution should be taken during periods of high rainfall, and swimming avoided if water is discoloured. Sites are monitored weekly and warning signs erected if water quality deteriorates.
Poor
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have generally poor water quality (see Table D2 for details). These sites receive run-off from one or more of the following sources and may contain animal or human faecal material:
- tertiary treated wastewater
- urban stormwater, marinas or moorings, intensive agriculture
- river discharges containing untreated / primary / secondary treated wastewater or on-site waste treatment systems
- river discharges impacted by tertiary treated wastewater, combined sewer overflows, intensive agricultural/rural catchments, feral bird/animal populations.
Recommendation: Generally not okay for swimming, as indicated by historical results. Swimming should be avoided, particularly by the very young, the very old and those with compromised immunity. Permanent warning signs may be erected at these sites, although councils may monitor these sites weekly and post temporary warnings.
Very poor
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have very poor water quality (see Table D2 for details). These sites receive run-off from one or more of the following sources and may contain animal or human faecal material:
- untreated/primary/secondary treated wastewater
- on-site waste treatment systems
- tertiary treated wastewater
- urban stormwater, marinas or moorings, intensive agriculture
- river discharges containing untreated/ primary/secondary treated wastewater or on-site waste treatment systems.
Recommendation: Avoid swimming, as there are direct discharges of faecal material. Permanent signage will be erected at the beach stating that swimming is not recommended.
Note H(vii): Catchment Assessment Checklist for freshwater recreational areas
Catchment Assessment Checklist for freshwater recreational areas [PDF, 296 KB]
Figure H3: Sanitary Inspection Category for freshwater sites
Note H(viii): Microbiological Assessment Category for freshwater recreational areas
The Microbiological Assessment Category is calculated on the basis of five years of historical data (at least 100 data points). Data collected during or immediately following rainfall, as part of routine sampling, should be included in the calculation of the MAC. The purpose of the MAC is to give an indication of general water quality over an extended period, to allow for variations in climatic conditions. The MAC is used in conjunction with the Sanitary Inspection Category (SIC) to determine the Suitability for Recreation Grade, and to confirm that the selected SIC is accurate, based on historical water-quality results.
Note: Follow-up samples from an alert or action mode response should not be included in the data used to generate an MAC. If using the software provided by the Ministry for the Environment to generate grades, follow-up will need to be removed from the dataset prior to importing.
See Section E.3 for MAC definitions for freshwater.
Note H(ix): Suitability for recreation grade for freshwater recreational areas
Explanation of grades
Beaches are graded by considering microbiological monitoring results from previous years in combination with the factors in the catchment that may contribute faecal contamination to the beach. It is a risk-associated grading of the beach, meaning that it provides an indication of what the likely condition of the beach will be on any day. The following general explanation provides a description of each of the beach grades.
Very good
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have very good water-quality (see Table E2 for details). This indicates there may be some indirect run-off from low intensity agricultural/urban/rural/bush catchments, but there are likely to be no significant sources of faecal contamination.
Recommendation: Considered satisfactory for swimming at all times, and therefore may not require monitoring on a regular basis.
Good
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have generally good water-quality (see Table E2 for details). On occasions (such as after high rainfall) there may be an increased risk of contamination from run-off. Such sites receive run-off from one or more of the following sources and may contain animal or human faecal material:
- river discharges impacted by tertiary treated wastewater, combined sewer overflows, sewer overflows, intensive agricultural/rural catchments, significant feral bird/animal populations
- river discharges impacted by; run-off from low-intensity agricultural/urban/rural catchment
- direct discharges from stormwater not contaminated by sewage, boat moorings or marinas
- direct discharges from low-intensity agriculture.
Recommendation: Satisfactory for swimming most of the time. Exceptions may include following rainfall. Such beaches are monitored regularly throughout the summer season and warning signs will be erected if water quality deteriorates.
Fair
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have generally fair water-quality (see Table E2 for details). However, events such as high rainfall increase the risk of contamination levels from run-off. Such sites receive run-off from one or more of the following sources and may contain animal or human faecal material:
- river discharges impacted by tertiary treated wastewater, combined sewer overflows, sewer overflows, intensive agricultural/rural catchments, significant feral bird/animal populations
- river discharges impacted by; run-off from low-intensity agricultural/urban/rural catchment
- direct discharges from stormwater not contaminated by sewage, boat moorings or marinas
- direct discharges from low-intensity agriculture.
Recommendation: Generally satisfactory for swimming, though there are many potential sources of faecal material. Caution should be taken during periods of high rainfall, and swimming avoided if water is discoloured. Sites are monitored weekly and warning signs erected if water quality deteriorates.
Poor
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have generally poor water-quality (see Table E2 for details). These sites receive run-off from one or more of the following sources and may contain animal or human faecal material:
- tertiary treated wastewater
- urban stormwater, intensive agriculture, unrestricted stock access, dense bird populations
- low-intensity agriculture, marinas or boat moorings, urban stormwater not contaminated by sewage
- river discharges containing untreated/ primary/secondary treated wastewater or on-site waste treatment systems
- river discharges impacted by tertiary treated wastewater, combined sewer overflows, intensive agricultural/rural catchments, feral bird/animal populations.
Recommendation: Generally not okay for swimming, as indicated by historical results. Swimming should be avoided, particularly by the very young, the very old and those with compromised immunity. Permanent warning signs may be erected at these sites, although councils may monitor these sites weekly and post temporary warnings.
Very poor
Water-quality tests and assessment of potential contamination sources indicate beaches within this category are considered to have very poor water-quality (see Table E2 for details). These sites receive run-off from one or more of the following sources and may contain animal or human faecal material:
- untreated/primary/secondary treated wastewater
- on-site waste treatment systems
- tertiary treated wastewater
- urban stormwater, intensive agriculture, unrestricted stock access, dense bird populations
- river discharges containing untreated/ primary/secondary treated wastewater or on-site waste treatment systems.
Recommendation: Avoid swimming, as there are direct discharges of faecal material. Permanent signage will be erected at the beach stating that swimming is not recommended.
Note H(x): Application of grades and single samples
The risk of becoming sick from swimming at a beach is inferred from the associated grade. Beaches graded Very Good almost always pass the Microbiological Water Quality Guidelines, and there are few sources of faecal contamination in the catchment. Consequently, the risk of becoming sick is low. Beaches graded Very Poor are within catchments with significant sources of faecal contamination, and they rarely pass the guidelines. The risk of becoming sick at these beaches is high and swimming is not recommended. Unless there is a change in the catchment characteristics of beaches graded Very Poor, monitoring is not justified.
For the remaining grades of beaches (Good, Fair, Poor), water quality deteriorates and the risk of illness from swimming increases down the gradient from Good to Poor. The conditions affecting water quality vary (e.g. Good beaches usually pass the guidelines, but occasions such as high rainfall increase the risk of contamination from run-off).
For these beaches it is recommended that weekly monitoring be carried out during the bathing season. The public will be informed when swimming is not recommended (when a sample taken from the beach exceeds the action-level single-sample criteria of the Microbiological Water Quality Guidelines).
Note H(xi): Interim grading
An interim grade is provisional, and dependent on annual review as additional information becomes available until five years of data is obtained. An interim grade is mainly for management purposes, although it may be communicated to the public if it is clearly defined as interim only.
An interim grade can be derived using less than the recommended five years’ data where at least 20 data points over the period of greatest recreational use are available. This period will normally be the summer bathing season, but may vary with the types of recreational activity most common in the area.
Circumstances under which an interim grade might be applied include:
- where the data available is incomplete, either with respect to the MAC, or the SIC, or both
- where there is reason to believe that the existing grading no longer accords with changed circumstances, but the data required for completing the grading is insufficient.
Note H(xii): Modifying beach grades
Modifying a beach’s SFRG is justified where occasional and predictable contamination events are identified, and interventions can be demonstrated to be effective in discouraging recreational use. Sites with a modified SFRG should be labelled, and their condition and the effectiveness of management interventions assessed annually.
Modifying an SFRG is particularly relevant to mid-range beaches (Good, Fair and Poor) and where there is disagreement between the SIC and MAC (i.e. a ‘Follow Up’). The process for modifying a beach grade is as follows.
- Determine whether contamination events are occasional and predictable (i.e. triggered by an event such as heavy rainfall).
- Implement and evaluate the effectiveness of management interventions to discourage recreational use during known high-risk periods.
- Reassess the SIC, removing the source of predictable contamination events (provided interventions are effective).
- Reassess the MAC (where there is sufficient data), excluding results caused by the trigger event.
- Modify the beach grade according to the revised SIC and MAC.
Data requirements for modifying an SFRG
To reassess the MAC, rainfall-related data should be identified and removed from the dataset. This requires all rainfall data to be marked for easy identification in subsequent years. If removing rainfall data decreases the size of the dataset below the 100 required to generate a MAC, it cannot be modified. Sampling in the subsequent season may be sufficient to generate the required number of samples to reassess the MAC. If not, councils should design a programme to meet this requirement, or stick with modifying the SFRG based on the revised SIC category only. Once sufficient data has been collected the MAC can be reassessed and the SFRG modified accordingly.
The following example illustrates how to modify a grade.
Box 5: Example of modifying a beach grade
Initial assessment of the site resulted in a SIC of High (primary impact = ‘stormwater outlets with potential sewage contamination’) and a MAC of C (95 percentile = 315), giving an SFRG of Poor.
The stormwater overflows are caused by heavy rainfall, and are therefore predictable events. Signs were introduced to warn against swimming for up two days following rainfall. Site monitoring over the following season found public warnings to be effective in deterring use of the site for up to two days following rainfall.
As a result, sewage impacted stormwater was replaced as the primary impact on the site with stormwater protected from sewage ingress. This improved the SIC from High to Moderate and gave a modified SFRG of Fair (but unsuitable for two days after heavy rainfall).
Water-quality sampling confirmed that after two days microbiological levels returned to pre-rainfall levels. After removing rainfall data, there were insufficient results to generate a MAC. A sampling strategy was designed for the following season to collect sufficient samples to meet the 100 data points needed. Reanalysis of water-quality data using water quality to which people were exposed revealed a 95 percentile of 126, improving the MAC from C to B.
The modified grade for the site becomes Good (but unsuitable for two days after heavy rainfall), given the modification of both the SIC and MAC.
Note: Remediation of stormwater overflows would result in an SFRG of Good, based on the outcome of the modified grade.
Demonstrating effectiveness of management interventions
Management interventions may range from warning signs to public notices in newspapers. They should aim to reduce beach usage under specific conditions that are known to cause contamination, e.g. after heavy rainfall. It is critical that the effectiveness of these interventions be demonstrated before a beach’s SFRG can be modified. This requires management interventions to be in place for at least one bathing season before a site’s grade can be modified.
The effectiveness of management interventions can be assessed by measuring the decrease in beach use following their implementation. An 80% reduction in recreational use is required for management interventions to be considered effective. Head counts are available from surf clubs to provide baseline information. If no surf club is present, councils or health agencies should collect their own information on beach usage.
Before modified grades are finalised, the monitoring authority should consult other councils and the Medical Officer of Health in their area to gain agreement on the outcome of the regrading. Given their public health protection role, the Medical Officer of Health in particular should concur that:
- there is sufficient documentation to support the original Suitability for Recreation Grade
- there is evidence that management interventions have been effective
- the modified grade is appropriate for the site.
What information to report?
Where site grades have been modified, regional and local councils will report the modified grade to the public. The modified grade provides information on the condition of the site, including when it is not suitable for recreational use (i.e. Good – except for two days following rainfall). While the ‘actual’ water quality at the site hasn’t been improved by removing the source of contamination, the risk has been mitigated through effective management interventions.
The Ministry for the Environment is interested in reporting the original SFRGs, as these reflect the actual water quality and potential for faecal contamination. Reporting the original SFRG will enable the Ministry to pick up improvements to the overall condition of beaches as a result of infrastructural or landuse changes over time.
Note H(xiii): Percentile guideline values for seawater (WHO 2001) and freshwater
Seawater
For marine waters, only faecal streptococci (enterococci) showed a dose–response relationship for both gastrointestinal illness (Kay et al 1994) and Acute Febrile Respiratory Infection (AFRI) (Fleisher, Kay, Salmon et al 1996). A recent reanalysis of this data (Kay et al 2001) using a range of contemporary statistical tools has confirmed that the relationships originally reported are robust to alternative statistical approaches.
The guideline values for microbiological quality given in Table H1 are derived from the key studies described in the previous paragraph.
The cut-off or bounding values (40, 200, 500) are expressed in terms of the 95th percentile of numbers of faecal streptococci per 100 mL, and represent readily understood levels of risk, based on the exposure conditions of the key studies.
For the purposes of water-quality monitoring, the terms ‘faecal streptococci’, ‘intestinal enterococci’ and ‘enterococci’ are considered to be synonymous (Figueras et al 2000). Exposure to recreational waters with these measured indicators refers to body contact that is likely to involve head immersion, such as swimming, surfing, white-water canoeing, scuba diving and dinghy-boat sailing.
Table H1: Guideline values for microbiological quality of marine recreational waters
| 95th percentile value of enterococci/ 100 mL (rounded values) | Basis of derivation | Estimated risk |
|---|---|---|
| =< 40 | This value is below the NOAEL in most epidemiological studies. | < 1% GI illness risk, < 0.3% AFRI risk. This relates to an excess illness of less than one incidence in every 100 exposures. The AFRI burden would be negligible. |
| 41–200 | The 200/100 mL value is above the threshold of illness transmission reported in most epidemiological studies that have attempted to define a NOAEL or LOAEL for GI illness and AFRI. | 1–5% GI illness risk, 0.3–< 1.9% AFRI illness risk. The upper 95th percentile value of 200 relates to an average probability of one case of gastroenteritis in 20 exposures. The AFRI illness rate at this water quality would be 19 per 1000 exposures, or approximately 1 in 50 exposures. |
| 201–500 | This level represents a substantial elevation in the probability of all adverse health outcomes for which dose–response data is available. | 5–10% GI illness risk, 1.9–3.9% AFRI illness risk. This range of 95th percentiles represents a probability of 1 in 10 to 1 in 20 of gastroenteritis for a single exposure. Exposures in this category also suggest a risk of AFRI in the range of 19–39 per 1000 exposures, or a range of approximately 1 in 50 to 1 in 25 exposures. |
| > 500 | Above this level there may be a significant risk of high levels of minor illness transmission. | > 10% GI illness risk, > 3.9% AFRI illness risk. There is a greater than 10% chance of illness per single exposure. The AFRI illness rate at the 95th percentile point of 500 enterococci per 100 mL would be 39 per 1000 exposures, or approximately 1 in 25 exposures. |
Source: Adapted from WHO 2001.
Notes:
- AFRI = acute febrile respiratory illness; GI = gastrointestinal; LOAEL = lowest observed-adverse-effect level; NOAEL = no-observed-adverse-effect level.
- The ‘exposure’ in the key studies was a minimum of 10 minutes’ bathing involving three immersions. It is envisaged that this is equivalent to many immersion activities of similar duration, but it may underestimate risk for longer periods of water contact or for activities involving higher risks of water ingestion (see also note 7).
- The ‘estimated risk’ refers to the excess risk of illness (relative to a group of non-bathers) among a group of bathers who have been exposed to faecally contaminated recreational water under conditions similar to those in the key studies.
- The functional form used in the dose–response curve assumes no excess illness outside the range of the data (i.e. at concentrations above 158 faecal streptococci/100 mL). Thus, the estimates of illness rate reported above are likely to be underestimates of the actual disease incidence attributable to recreational-water exposure.
- This table would produce protection of ‘healthy adult bathers’ exposed to marine waters in temperate north European waters.
- It does not relate to children, the elderly or immunocompromised people, who would have lower immunity and might require a greater degree of protection. There is no available data with which to quantify this, and no correction factors are therefore applied.
- Epidemiological data on freshwaters or exposures other than bathing (e.g. high-exposure activities such as surfing, dinghy-boat sailing or white-water canoeing) are currently inadequate to present a parallel analysis for defined reference risks. Thus, a single microbiological value is proposed, at this time, for all recreational uses of water, because insufficient evidence exists at present to do otherwise. However, it is recommended that the severity and frequency of exposure encountered by special interest groups (such as bodysurfers, board riders, windsurfers, sub-aqua divers, canoeists and dinghy sailors) be taken into account.
- Where disinfection is used to reduce the density of indicator bacteria in effluents and discharges, the presumed relationship between faecal streptococci (as indicators of faecal contamination) and pathogen presence may be altered. This alteration is, at present, poorly understood. In water receiving such effluents and discharges, faecal streptococci counts may not provide an accurate estimate of the risk of suffering from mild gastrointestinal symptoms or AFRI.
- Risk attributable to exposure to recreational water is calculated after the method given by Wyer et al (1999), in which a log 10 standard deviation of 0.8103 was assumed. If the true standard deviation for a beach were less than 0.8103, then reliance on faecal streptococci would tend to overestimate the health risk for people exposed above the threshold level, and vice versa.
- Note that the values presented in this table do not take account of health outcomes other than gastroenteritis and AFRI. Where other outcomes are of public health concern, then the risks should be assessed and appropriate action taken.
- Guideline values should be applied to water used recreationally and at the times of recreational use. This implies care in the design of monitoring programmes to ensure that representative samples are obtained. It also implies that data from periods of high risk may be ignored if effective measures were in place to discourage recreational exposure.
Freshwater
The marine water guideline values have been derived from epidemiological studies, but this type of study is seldom carried out for freshwater and has not been conducted for New Zealand. Instead values are based on a quantitative risk assessment for Campylobacter infection using the results obtained in a recent nationwide study (McBride, Till, Ryan et al 2002). Campylobacteriosis accounts for more than half of New Zealand’s burden of notifiable disease, and for this reason it was selected as the end point for this analysis. Also in that study a reasonable correlation was found between concentrations of Campylobacter and of E. coli.
Table H2: Guideline values for microbiological quality of freshwater recreational waters
| 95th percentile value of E. coli/ 100 mL(rounded values) | Basis of derivation | Estimated risk of Campylobacter infection |
|---|---|---|
| =< 130 | This value is the NCRL for Campylobacter infection. | < 0.1% occurrence. This relates to less than one case of Campylobacter infection in every 1000 exposures. |
| 131–260 | The 260/100 mL value is above the threshold of Campylobacter infection (above the NCRL). | 0.1–1% occurrence. The upper 95th percentile value of 260 relates to an average probability of one case of Campylobacter infection in every 100 exposures. |
| 261–550 | This level represents a substantial elevation in the probability of Campylobacter infection compared to the New Zealand background rate. | 1–5% occurrence. This range of 95th percentiles represents a probability of 1 in 100 to 5 in 100 of Campylobacter infection. |
| > 550 | Above this level there may be a significant risk of high levels of Campylobacter infection. | > 5% occurrence. The upper 95th percentile value of 550 represents a greater than 1 in 20 chance of Campylobacter infection. |
Notes:
- NCRL = no-calculated-risk level. This is based on the 55th percentile of E. coli distributions because the calculated community Campylobacter risk at a given recreational site starts to rise above zero at this percentile. (See the all-data-for-all-catchments case Tables A3.3.2 and A3.7.3 in the Freshwater Microbiology Research Programme Report (FMRPR), Pathogen Occurrence and Human Health Risk Assessment Analysis (McBride et al 2002).)
- The routes of infection include both ingestion and inhalation from contact recreation with mode (most likely value) for duration = half hour, and volume ingested/inhaled =50 mL (Monte Carlo modelling of health risk, FMRPR). This may underestimate risk for longer periods of water contact or for activities involving higher risk of water ingestion (e.g. higher exposure activities such as dinghy-boat sailing or white-water canoeing). It is recommended that the severity and frequency of exposure encountered by special interest groups be taken into account.
- The “estimated risk” refers to the community risk at a given recreational site (1000 people at the same beach each day) of Campylobacter infection (Table A3.7.3 in the FMRPR) from exposure to faecally contaminated recreational water similar to the 25 sites in the Freshwater Microbiological Research Programme.
- These risks does not relate to children, the elderly or immunocompromised people, who would have lower immunity and might require a greater degree of protection. There is no available data with which to quantify this, and no correction factors are therefore applied.
- Where disinfection is used to reduce the density of indicator bacteria in effluents or discharges, the presumed relationship between E. coli (as indicators of faecal contamination) and pathogen presence may be altered. This alteration is, at present, poorly understood. In waters receiving such effluents and discharges, E. coli may not provide an accurate estimate of the risk of infection.
- Note that the values presented in this table do not take account of health outcomes other than the risk of Campylobacter infection. Where other outcomes are of public health concern, the risks should be assessed and appropriate action taken.
- Guideline values should be also applied to waters at the time of recreational use. This implies care in the design of monitoring programmes to ensure representative samples are obtained. It may also imply that data from periods of high risk may be ignored if effective measures are in place to discourage recreational exposure.
Note H(xiv): Derivation of alert and action levels for seawater and freshwater
The alert and action levels are management tools, ensuring that risks are kept below illness risks of about 2% per 1000 swimmers. They represent, respectively, 80% and 90% one-sided upper tolerance limits, assuming that the waters are borderline for compliance with previous guidelines and a stated variability applies (measured as the standard deviation of logarithms).
See Appendix 2: Developing the Guidelines.
Note H(xv): State of the environment analysis and reporting
Monitoring and reporting the state of the environment
This section discusses the Ministry’s Environmental Monitoring and Reporting system, which uses environmental performance indicators to report on the state of the environment. The Microbiological Water Quality Guidelines for Marine and Freshwater Recreational Areas serve as the monitoring protocol for the marine and freshwater recreation indicators. In this document the monitoring approach, analysis and data management procedures are described to ensure the generation of robust information for reporting of the indicators.
Good-quality information is increasingly important for central and local government to meet public expectations, be accountable and demonstrate performance. Information is used to produce State of the Environment reports; to review national legislation, regional and district plans; to assess compliance of resource consents; for environmental education, and for the strategic and annual planning process.
Partnerships for monitoring and reporting
The Ministry for the Environment has been working with Regional, City and District Councils, Medical Officers of Health and the Ministry of Health to develop approaches for monitoring and reporting the state of recreational beaches.
Should the Ministry for the Environment want to use the information generated for National State of the Environment reporting then the Ministry would work in partnership with Councils to agree on the principles for information sharing.
Software
The Ministry for the Environment has developed software to assist councils with the process of grading beaches, and calculating the two state of the environment indicators. The software (Bathewatch.exe) follows the same format as the guidelines and uses historical data and information from the Catchment Assessment Checklist to calculate the Microbiological Assessment Category and the Sanitary Inspection Category. The MAC and SIC are used to generate a Suitability for Recreation Grade and percentage compliance with the guidelines for the site.
The software and a user guide can be downloaded from the Ministry’s website.
Data storage and archiving
Most councils store their data as Excel files. The user guide for the Bathewatch software specifies the data file format requirements for loading data into the software. For the MAC component of the SFRG assessment, the data collected from field observations must be stored in a comma-delimited value (*.csv) file format. The data must be stored in this specific file format or it will fail to load properly. It is a simple process to convert files from an Excel format into a *.csv format. The procedure is detailed in the Bathewatch user guide.
It is expected that councils will archive their monitoring data using the council’s normal computer back-up system. The council may wish to consider burning the data onto a CD or an otherwise secure file.
Note H(xvi): Reporting to the public
Public health reporting
If exceedances of alert and/or action levels are recorded during weekly monitoring of recreational beaches, the appropriate responses should be undertaken, as described in section D.4 of the guidelines and Note H(xvii) of these notes.
State of the Environment reporting
The two beach water quality indicators can be reported using the data generated by councils. For:
- the percentage of monitored beaches in each beach grade
the indicator provides a measure of the general state of bathing beaches by combining the risk of contamination from the catchment with the microbiological monitoring at the beach. It reports the overall suitability of beaches for bathing. Beaches will be classified into one of five grades (from very good to very poor).
And for:
- the percentage of the season beaches or coastal areas are suitable for bathing or shellfish gathering
the indicator will give an indication of the amount of time in a season the water quality was considered suitable for bathing or shellfish gathering. It provides a measure of the variation of microbiological quality of bathing waters within a bathing season.
Indicator fit with the pressure-state-response model
The Ministry for the Environment has used the pressure-state-response (PSR) model for developing environmental performance indicators – refer to Note G(iii): State of the Environment Reporting, page G3.
The indicators on which these guidelines are based – percentage of monitored beaches in each beach grade, and percentage of the season beaches or coastal areas were suitable for contact recreation or shellfish gathering – are state indicators that provide general information on the public health risk presented by recreational waters. Pressure indicators would measure the surrounding land use and discharges to water to assist identification of potential causes of changes in water quality. Response indicators would identify management or policy changes (e.g. infrastructural improvements, land-use management policies, national environmental standards) to manage issues for recreational waters.
Note H(xvii): Management responses to exceedances for marine and freshwater
The planned responses to exceedances of the guidelines should be considered and documented when establishing a regional monitoring protocol, and communicated to all agencies that will have a role to play (e.g. regional councils, territorial local authorities and health agencies). Documentation should clearly state who is responsible for carrying out what actions in response to exceedances. If the response varies from site to site, depending on the overall grade, this should also be clearly stated.
See Section B for details on who monitors and reports.
Single-sample exceedances
The point of having single-sample limits is to identify variations in water quality within the bathing season that pose an immediate risk to human health.
There are two levels of response to single-sample exceedances.
Alert mode
The first is alert (or amber) mode, and is triggered when a single sample is greater than 140 enterococci per 100 mL for marine waters and 260 E. coli per 100 mL for freshwaters. In this situation, sampling should be increased to daily to improve the information base and identify whether or not the problem is ongoing. A catchment assessment should be carried out to identify all possible sources of contamination. The monitoring authority should inform the Medical Officer of Health and the other council(s) (either regional or local, depending on who is doing the monitoring).
Action mode
The second level of response to a single-sample exceedance is action (or red) mode. In the case of marine waters this is triggered when two consecutive samples are greater than 280 enterococci per 100 mL, and for freshwaters when a single sample exceeds 550 mL E. coli per 100 mL. In this instance the monitoring authority informs the Medical Officer of Health and the other council(s) of the problem. Sampling is increased to daily and a catchment assessment carried out to identify the source of the contamination. The public should be notified of the health risks using appropriate methods identified in the regional monitoring plan. Discussion between the regional council, territorial local authority and Medical Officer of Health should take place to ascertain who is responsible for fixing the problem.
The Ministry for the Environment and Ministry of Health have developed sign templates in consultation with councils and health agencies to use in response to exceedance events and at high-risk sites. (See Appendix 3 for these sign templates.)
High-risk sites
High-risk sites are those sites graded Poor or Very Poor, and will generally have direct discharges, such as sewer outfalls, impacting on them. While the guidelines and notes provide details on assessing these sites and recommend that permanent signs be erected to warn the public of the health risks (see Appendix 3 for sign templates), there is no discussion on remediation work. The agencies responsible for managing the infrastructure or land use affecting water quality, and those responsible for monitoring the sites and public health protection, may wish to discuss and document the remediation work required, and the timeframes, budgets, etc, for achieving this.
Communicating health risks
Communicating health risk is required after exceedance of the action level of the guidelines, as monitoring has identified increased levels of faecal material, which mean the site is unsuitable for recreational use. In order to protect public health, local authorities are required to notify the public of those health risks until the problem has been remedied.
When to issue warnings
The guidelines identify an action level, at which point use of a recreational site is considered unsuitable for contact recreation. For marine waters this is when two consecutive samples taken are greater than 280 enterococci per 100 mL, and for freshwaters when a single sample exceeds 550 E. coli per 100 mL. Warnings should be issued as soon as possible after the results from the sample are available. If contamination is obvious and likely to be ongoing, it is not necessary to wait for results from samples before issuing a health warning.
Other agencies involved in monitoring and reporting should be notified of exceedances before notifying the public of health risks.
Who to contact
The regional monitoring plan will clearly define lines of communication and responsibilities, such as whose role it is to notify the public. Results should be communicated as soon as possible to the agency responsible for public notifications.
What messages to convey
There are several messages to consider when issuing warnings, other than that there is a health risk. These are:
- there is a health risk
- the council is investigating the cause of the problem (i.e. the council is on to it)
- a list of alternative beaches to visit in the region
- an announcement when the problem has been fixed.
How to deliver the message
There are many ways to communicate information to the public. A number of factors will determine the methods chosen to deliver the warnings, including:
- the urgency of the message
- how well informed the community is
- the demographic make-up of the community.
The public awareness and education section provides more detail on establishing the best methods of delivering messages to the public (see Appendix 1), but the most widely used methods for health warnings are:
- signs
- newspaper articles
- radio
- notices in local shops
- websites
- 0800 numbers.
Signs
The Ministry for the Environment and Ministry of Health have developed sign templates in consultation with regional councils, local authorities and public health agencies. These are provided in Appendix 3.
Fact sheets
Fact sheets have been written to help communicate information about the guidelines and monitoring programmes. These generic fact sheets can be used for media releases, handing out at public at meetings, etc.
See Appendix 5 for fact sheets on different topics.
Summary
The most important messages to get across are:
- the health risk
- the council is responding quickly to the event.
It is also important to convey the unpredictable nature of this type of problem and the difficulties in isolating the cause.
Once the problem has been fixed, the public should be notified. This will be apparent from the removal of signs, but should be highlighted through use of the media, community meetings, and contact with user groups, etc.
The public education and awareness programme outline (Appendix 1) provides more information on engaging public support for the monitoring programme.
Management interventions for modified grades
Management interventions will vary in type according to the nature of the predictable event leading to the modification and the target audience. Interventions may range from permanent warning signs on beaches, to public meetings (see Appendix 1: Public Education and Awareness Programme Outline). The ability to demonstrate the effectiveness of interventions in discouraging the public from using the site during periods of high risk is critical. This is what will lead to a modified grade. How this is assessed will vary, but must be verified by the Medical Officer of Health.
Part III: Explanatory Notes to the Guidelines
June 2003
© Ministry for the Environment